What Are the New Childhood Epidemics?
While you may not hear about it on the news or at your doctor’s office, we are currently witnessing one of the most devastating health epidemics of all time. This is a health epidemic that first showed up in children living in modern industrial areas like the U.S. and in Europe but is increasingly affecting children around the globe. It threatens the very future of human life on the planet. This epidemic includes chronic health conditions like asthma, allergies, and autoimmune diseases, and it also includes developmental or neurobehavioral conditions such as autism, ADHD, sensory processing disorders, and learning disabilities. Collectively, we call these the “new childhood epidemics,” because they are unlike anything we have seen before, and they are impacting children in breathtaking numbers.
We don’t actually have an updated statistic on exactly how many children are affected, but it is believed that this chronic illness and developmental health epidemic affects more than half of U.S. children. The statistic that is often cited to provide some understanding of the state of children’s health in America is from a paper that was published in 2011. Christina Bethel et al. of Johns Hopkins reported in a 2011 paper that at least 54% of U.S. children in the U.S. had a chronic health or developmental condition. Much of the data cited in that paper is from the early 2000s! Given the rate at which chronic health and developmental conditions have grown over the last few decades, up from an estimated 2% of children diagnosed with a chronic illness in the 1960s, we estimate that it may be as high as 70% or more of children.
We must start asking the questions:
- Why do at least 1 in 9 children have ADHD?
- Why do nearly 30% of children have an allergy, with 1 in 13 having an anaphylactic food allergy?
- Why do at least 8% of children have asthma?
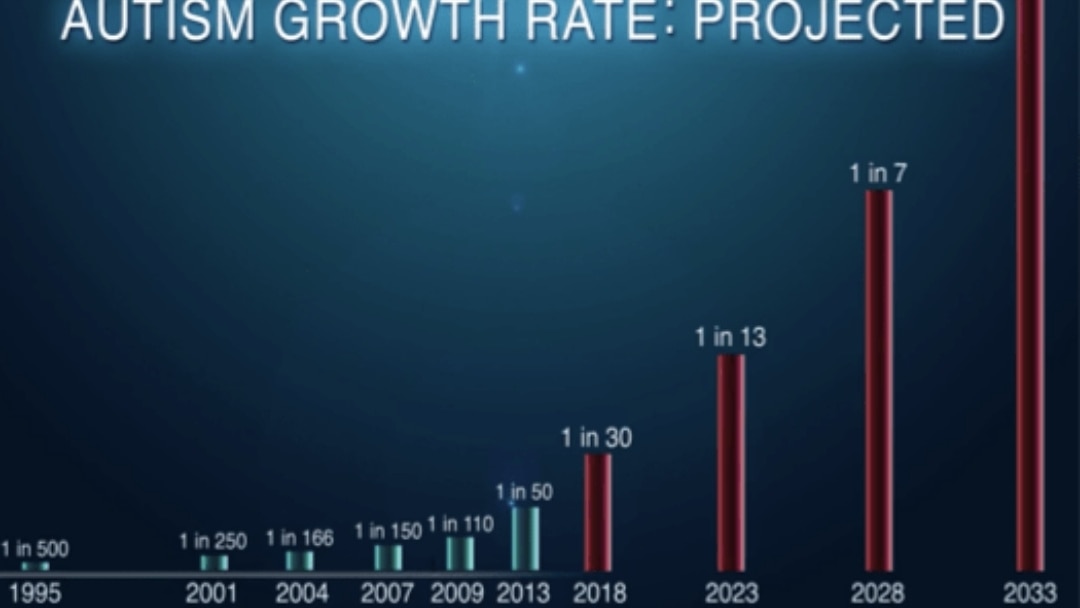
- Why does 1 in 30 children have autism?
In addition to the children representing these statistics, many children who don’t carry an official diagnosis live with daily troubling symptoms such as chronic constipation, sensory sensitivities, severe anxiety, behavioral challenges, chronic throat clearing or tics, chronic runny nose or sinus congestion, skin rashes, picky eating and other “soft signs” of being affected by this epidemic.
Ask anyone over 45 or anyone who is a grandparent whether they remember children having so many symptoms and diagnoses. They will tell you that it wasn’t like this when they were growing up. School nurses’ offices weren’t lined with epi-pens and inhalers. There was little need for IEPs (Individualized Education Plans) for children with special needs or learning challenges. Most people had never even heard the word autism and didn’t know anyone who had the symptoms and stereotypical behaviors of autism (such as echolalia, hand flapping, stimming, sensory aversion, inability to speak, and more).
What Has Changed?
Many conventional medical experts will tell you that these diagnoses are genetic in origin. Or when pressed to acknowledge that genes don’t mutate quickly enough to explain the escalation of cases, you will often hear them rationalize that, “I think we are just better at diagnosing.” While that may be true for some of the more subjective diagnoses such as autism and ADHD, especially when they are milder versions that could theoretically have been missed decades ago, it can’t be true for diagnoses that are objectively diagnosed such as life-threatening food allergies, type 1 diabetes, asthma, obesity or autoimmune disease. It certainly can’t explain the increase in conditions like profound (or level 3, severe) autism that requires round-the-clock care from caregivers.
Yet, we are seeing a rise in all these diagnoses. Every single one! When pressed further with these facts, experts might begin to acknowledge “gene environment interaction” though they won’t necessarily be able to tell you what environmental factors are triggering this interaction with our children’s genes, outside of some very vague references to air pollution, plastics, sedentary lifestyles or other nonspecific “environmental factors.”
The truth is that this epidemic is moving so quickly that the “experts” we tend to rely on for answers to problems like this just haven’t been able to keep up with the emerging science. But Documenting Hope has, because this is our singular area of focus. This is what we believe to be the most pressing issue of our time. Moms and dads of affected kids are truly motivated to uncover the root causes of this devastating epidemic. They know the truth of what they are experiencing, and they have real skin in the game to reverse this trend for their own children’s sake and others.
Root Causes
If you want to know why there are so many kids with acid reflux, failure to thrive, developmental delays, chronic ear infections, or chronic constipation if you seek to understand what is contributing to the skyrocketing rates of autoimmune disorders, autism, ADHD, asthma, Sensory Processing Disorder and PANS/PANDAS, then you need to take a hard look at how we are living in the modern world and how much it differs from how people lived even a few decades ago.
Our world is so different than the world our parents and grandparents grew up in and the things we eat, breathe, think, and do on a daily basis are profoundly impacting our kids’ health.
If your children have diagnoses or chronic symptoms (or are just showing the “soft signs” of being affected), you will soon find out that there are certain imbalances in the body, caused by the totality of modern living, that may be preventing them from reaching their full potential. To be sure, there are some very specific environmental factors (antibiotics or specific herbicides like glyphosate, for example) that play a more significant role in causing or triggering many of these conditions, and it is also true that there are many paths to chronic health and developmental conditions. Each child has arrived at their diagnosis via their own bioindividual and unique set of environmental variables and yes, a variety of genetic factors that can often be best supported through thoughtful diet and lifestyle changes and even used to reverse symptoms.
Different Recipe, Same Dish
Let’s take autism, for example. There is no singular path to the development of autism. Think of the analogy of how many different recipes can be used to arrive at the same dish, say, “chili.” Even though different recipes were used, everyone ends up with a bowl of chili:
- One recipe contained tomatoes, kidney beans, and ground beef (analogies for variables like antibiotics, chemical exposures, stress).
- Another recipe had mostly tomatillos, black beans, and chicken (analogies for variables like pesticides, polycarbons from food, genetic susceptibility).
- Another chili was made with garbanzo beans, zucchini and lots of different types of hot peppers (mercury-laden air pollution, viral infections, multiple genetic vulnerabilities).
Some recipes may have been made quickly; others had to slowly simmer for a long time “to become chili.”
Even though the ingredients and steps varied, all those different recipes still created a dish that we call chili. Some chilis will be very intense and spicy, and some will be mild, bland or hard to describe, just “chili-like.”
The important part is this: the categories of ingredients (proteins, beans, spices, vegetables) or modern stressors (toxins, infections, poor diet, stress, disrupted microbiome, etc.) are similar. Taking the analogy of recipes further, if two people are diagnosed with rheumatoid arthritis, their exact health stressors or adverse exposures may not be the same, but generally speaking, the categories of stressors will be similar: chemical toxins like heavy metals, infections like the Epstein Barr virus, poor diet, stress, microbiome shifts. Those who are really paying attention to these health trends are seeing familiar patterns. The exact combinations of ingredients within each category differ from person to person, but the “end product” may look the same to doctors whether it’s rheumatoid arthritis, autism or another chronic condition.
No two children develop a condition for the exact same reason, under the exact same circumstances. There are hundreds and thousands of variables that determine a particular child’s health outcomes. This is why it is so hard for the medical and scientific community to land on one answer for a particular diagnosis or to explain why our children are so sick.
What the science is now suggesting over and over, and what many parents are observing, is that the root causes of this epidemic are all tied to the way we live in the modern world. The exact recipe that constitutes one person’s chili or “bakes their cake” or gives them their symptoms and diagnosis is different from someone else’s, but the basic ingredients all came from the same sources – some combination of a “pantry of ingredients” that doesn’t serve the health of its consumers, especially those most vulnerable, our developing children.
The good news is that many of the root causes of today’s childhood epidemics include categories such as toxicity, birth trauma, gut dysbiosis and nutritional deficiencies are treatable, and the conditions are even reversible.
Are We Facing a National Security Crisis?
In 2010, a project called Mission Readiness, led by America’s Retired Generals, Admirals and Civilian Military Leaders, released a very concerning report titled “Too Fat to Fight”. Citing Department of Defense data, this report indicated that:
“An alarming 75 percent of all young Americans 17 to 24 years of age are unable to join the military because they failed to graduate from high school, have criminal records, or are physically unfit.”
The vast majority of young people in America, the youth that are supposed to be at the peak of physical fitness and health, are so sick, mentally and physically, that they aren’t even able to meet the bare minimum requirements to enroll in the U.S. armed services. These retired Generals and Admirals have sounded the alarm that we are facing a national security crisis of epic proportions if we do not begin to focus on improving the health of our children.
Genetic Determinism Still Dominates the Narrative
Many people still believe in “genetic determinism” in which our genes cause conditions and diseases. They think that genes are what causes autism or that a child develops an autoimmune disease because someone in the family also had an autoimmune disease. This is a rather myopic view of how disease actually happens. Genetic determinism is not consistent with the trends we are observing in families who have healed their children from chronic health conditions and diagnosis.
There is no doubt that genes play an important role in whether or not someone develops a condition. However, genes are only one part of the picture. Did you know that scientists now believe that there are up to 1,000 genes that are implicated in the development of autism? Did you also know that these genes are implicated in Parkinson’s, depression, Alzheimer’s, anxiety, ADHD and many more neuroinflammatory conditions? These shared or similar genetic patterns are less tied to “autism” or to “Alzheimer’s” than they are to biological processes, such as detoxification or inflammation pathways. What this tells us is that although genes don’t “cause” autism, they call our attention to the fact that the human body is simply not able to handle the overwhelming load of modern health and environmental stressors (total load) that sets inflammation in process and competes for our body’s limiting detoxification pathways.
Our environment is so laden with toxins and filled with health stressing exposures that ALL humans are going to manifest symptoms at one point or another, regardless of our unique genetic profiles. When this total load of stressors hits us early in our development, there will be a developmental component which might look like autism, ADHD or a learning disability. Sharon Hausman Cohen MD, a Harvard-trained physician and genomics expert, is known for saying, “Autism is not genetic. It’s genomic.” This means that our environment interacts with our genes. This leads to physiological signs, symptoms, and the breakdowns and imbalances we are witnessing today.
What Kinds of Environmental Influences Are Making Our Children Sick?
To understand which environmental factors are making our children so sick, it is helpful to look at the common underlying physiological (biomedical) imbalances that are seen in today’s children regardless of diagnosis. Whether they have an autoimmune disease like alopecia, a life-threatening food allergy or autism, they will all have common imbalances that are measurable and often treatable. Once we acknowledge these imbalances, we can begin to identify the environmental factors known to cause them. See the chart below for a high-level overview of some of the most common imbalances seen in today’s children and what in our environment can contribute to those imbalances.
Common Underlying Imbalance
Common Causes of This Imbalance
By looking at the types of exposures and stressors on the righthand side of the chart, you’ll see that most of those exposures come simply from living in the modern world, a world where we have a toxic industrial food system, an environment that is a toxic soup of synthetic consumer products, industrial pollution and a world where we no longer move in natural rhythms or live in sync with nature. In summary, our modern ways of living are not supportive of human life in a way that is practical, sustainable, or even ultimately enjoyable.
Okay, It’s the Environment. But Only Non-Controversial Environmental Exposures, Right?
Once the acknowledgement is made that the environment is the main villain in the “new childhood epidemics,” it seems we are only willing to acknowledge certain environmental variables. The “safe-to-assume” non-controversial ones like “air pollution,” “plastics” and “bisphenol A.” Some of the things that are affecting our children remain controversial and difficult to talk about, despite decades of scientific literature providing evidence of a connection. Pharmaceuticals seem off-limits to explore or discuss even though they are among the biggest culprits (see our CHIRP poster presentation that reviews the connection between antibiotics and any chronic inflammatory condition). For example, the childhood immunization schedule seems to be completely off-limits as a possible contributing factor, even though there is mounting evidence of its implication in immunological burden and immune priming that seems to play a role in the pathophysiology of many chronic childhood conditions.
We’re All Exposed to the Same Toxic Soup, So Why Do Some Kids Get Autism, Others Get Asthma, and Others Escape Any Conditions?
Much of why we develop health conditions is our bioindividuality, which takes into consideration our genetics, our family health history, our personal medical history and the timing and sequence of the “total load” of our environmental and health stressors, as well as our cultural biases and lifestyle habits. Children that experience a burden of environmental or health stressors (acute or compounding) during critical developmental windows (e.g., in utero to 3 years old) are more likely to manifest neurodevelopmental symptoms like those commonly seen in autism or ADHD. Those stressors can be acute, meaning that a child was exposed to a heavy burden of a particular stressor all at once, like mercury or lead, or they can be slow and compounding over time. This is why two children never develop autism or ADHD in the same way.
Some children do have certain features of their biology or physiology that make them more resilient and resistant to developing health conditions. They might have a more robust microbiome, or genetics that make them excellent detoxifiers. They may have other strong supports in place, such as a clean and nutritious diet that is toxin-free and a lifestyle more in tune with natures rhythms So, no two children are the same, and they are going to react differently to the similar environmental health stressors or “categories of ingredients.” See the charts below as an illustration of how the different mix of health-stressor exposures can result in very different outcomes in terms of diagnosis for a particular child. Child A developed hay fever and food allergies, whereas Child B developed autism.


Reprinted with permission: Beth Lambert, A Compromised Generation (2010)
Regardless of what your child’s particular exposures have been, all our children are experiencing a “perfect storm” of environmental factors that are disrupting or destroying their immune systems, affecting their growth and development, and preventing them from living a full life.
It Can Get Better – There IS Hope!
Once you know about some of the root causes of your child’s symptoms and diagnoses, you can work with healthcare practitioners that know how to address them.
Kids can get better.
Many even drop their diagnoses, even for something as seemingly permanent as autism.
There is hope.
If you have an affected child, start here.
You’ll learn that much of the power of getting your child healthier lies in your own hands. You can truly lower a child’s total load and its impact. You can follow a better “recipe” for success!
If you are like us, and you recognize the urgency of this moment — the fact that this epidemic is a social and financial crisis, a national security crisis, and a moral imperative–then join us as we work to create a brighter future for our kids.
About Beth Lambert
Beth Lambert is a former healthcare consultant and teacher. As a consultant, she worked with pharmaceutical, medical device, diagnostic and other health care companies to evaluate industry trends.
She is the author of A Compromised Generation: The Epidemic of Chronic Illness in America’s Children (Sentient Publications, 2010). She is also a co-author of Documenting Hope's Brain Under Attack: A Resource for Parents and Caregivers of Children with PANS, PANDAS, and Autoimmune Encephalitis. She is a co-author of Reversal of Autism Symptoms among Dizygotic Twins through a Personalized Lifestyle and Environmental Modification Approach: A Case Report and Review of the Literature, J. Pers. Med. 2024, 14(6), 641.

In 2009, Beth founded Documenting Hope and currently serves as Executive Director. Beth attended Oxford University, graduated from Williams College and holds a Masters Degree in American Studies from Fairfield University.
Still Looking for Answers?
Visit the Documenting Hope Practitioner Directory to find a practitioner near you.
Join us inside our online membership community for parents, Healing Together, where you’ll find even more healing resources, expert guidance, and a community to support you every step of your child’s healing journey.
Sources & References
Allergies. Centers for Disease Control and Prevention, National Center for Health Statistics. Accessed 26 Mar 2026.
Adebayo, O., et al. The changing face of diabetes in America. Emerg Med Clin North Am. 2014;32(2):319-27.
Akinbami, L.J., et al. Attention deficit hyperactivity disorder among children aged 5-17 years in the United States, 1998-2009. NCHS Data Brief. 2011(70):1-8.
Atladottir, H.O., et al. The increasing prevalence of reported diagnoses of childhood psychiatric disorders: a descriptive multinational comparison. Eur Child Adolesc Psychiatry. 2015;24(2):173-83.
Barrett, B. Substantial lifelong cost of autism spectrum disorder. J Pediatr. 2014;165(5):1068-9.
Bateman, C. Autism–mitigating a global epidemic. S Afr Med J. 2013;103(5):276-7.
Bayer, J.K., et al. The Cool Little Kids randomised controlled trial: population-level early prevention for anxiety disorders. BMC Public Health. 2011;11:11.
Bernfort, L., et al. ADHD from a socio-economic perspective. Acta Paediatr. 2008;97(2):239-45.
Berry, E.A., et al. National estimates of the inpatient burden of pediatric bipolar disorder in the United States. J Ment Health Policy Econ. 2011;14(3):115-23.
Bethell, C., et al. A National and State Profile of Leading Health Problems and Health Care Quality for US Children: Key Insurance Disparities and Across-State Variations. Academic Pediatrics, May–June 2011, Volume 11, Issue 3, Supplement, p. S22–S33.
Bipartisan Policy Center. Lots to lose how America’s health and obesity crisis threatens our economic future. Washington, D.C.: Bipartisan Policy Center, 2012.
Bolin K, Cawley JH. The economics of obesity. 1st ed. Amsterdam; Boston: Elsevier JAI; 2007. xxiii, 364 p.p.
Bouder, et al. Brief report: Quantifying the impact of autism coverage on private insurance premiums. J Autism Dev Disord. 2009;39(6):953-7.
Brune, M., et al. Secular trends in new childhood epidemics: insights from evolutionary medicine. BMC Med. 2013;11:226.
Buescher, A.V., et al. Costs of autism spectrum disorders in the United Kingdom and the United States. JAMA Pediatr. 2014;168(8):721-8.
Bunyavanich, S., et al. Peanut allergy prevalence among school-age children in a US cohort not selected for any disease. J Allergy Clin Immunol. 2014;134(3):753-5.
Chai, G., et al. Trends of outpatient prescription drug utilization in US children, 2002-2010. Pediatrics. 2012;130(1):23-31.
Classen, J.B. Review of evidence that epidemics of type 1 diabetes and type 2 diabetes/metabolic syndrome are polar opposite responses to iatrogenic inflammation. Curr Diabetes Rev. 2012;8(6):413-8.
Costello, E.J., et al. 10-year research update review: the epidemiology of child and adolescent psychiatric disorders: II. Developmental epidemiology. J Am Acad Child Adolesc Psychiatry. 2006 Jan;45(1):8–25.
Currie, J.M., et al. National Bureau of Economic Research. Mental health in childhood and human capital. Cambridge, MA: National Bureau of Economic Research; 2007. 31 p.p.
Data and Statistics on ADHD. Centers for Disease Control and Prevention. Accessed 26 Mar 2026.
Data and Statistics on Children’s Mental Health. Centers for Disease Control and Prevention. Accessed 2 Sep 2020.
Dave, D., et al. The effect of an increase in autism prevalence on the demand for auxiliary healthcare workers : evidence from California. Cambridge, MA: National Bureau of Economic Research; 2012. 37 p.p.
Demeneix, B., et al. Losing our minds: how environmental pollution impairs human intelligence and mental health. New York: Oxford University Press; 2014. xxiii, 284 pages p.p.
Douglas, B.L., et al. Washington Business Group on Health. Obesity an overview of an American epidemic. Washington, D.C.: Washington Business Group on Health,; 2002.
Dusetzina, S.B., et al. Treatment use and costs among privately insured youths with diagnoses of bipolar disorder. Psychiatr Serv. 2012;63(10):1019-25.
Erskine, H.E., et al. The global burden of conduct disorder and attention-deficit/hyperactivity disorder in 2010. J Child Psychol Psychiatry. 2014;55(4):328-36.
Fletcher, J., National Bureau of Economic Research. The effects of childhood ADHD on adult labor market outcomes. Cambridge, MA: National Bureau of Economic Research; 2013. 25 p.
Frieri, M. Asthma linked with rhinosinusitis: An extensive review. Allergy Rhinol (Providence). 2014;5(1):41-9
Gupta, R.S., et al. The Public Health Impact of Parent-Reported Childhood Food Allergies in the United States. Pediatrics. 2018 Dec;142(6). pii: e20181235.
Hegner, R., et al. The asthma epidemic: prospects for controlling an escalating public health crisis: a background paper. Washington, D.C.: National Health Policy Forum; 2000. 16 p.p.
Hodgkins, P., et al. Risk of injury associated with attentiondeficit/ hyperactivity disorder in adults enrolled in employer-sponsored health plans: a retrospective analysis. Prim Care Companion CNS Disord. 2011;13(2).
The Impact of Asthma. American Lung Association. Accessed 2 Sep 2020.
Jonas, B.S., et al. Psychotropic medication use among adolescents: United States, 2005-2010. NCHS Data Brief. 2013(135):1-8.
Kong., A.P, et al. Diabetes and its comorbidities–where East meets West. Nat Rev Endocrinol. 2013;9(9):537-47.
Lahiri, S., et al. Pharmaceutical Research and Manufacturers of America. The prevalence and cost of select chronic diseases. Falls Church, Va.: Lewin Group,; 2007.
Laron, Z. Interplay between heredity and environment in the recent explosion of type 1 childhood diabetes mellitus. Am J Med Genet. 2002;115(1):4-7.
Lavelle, T.A., et al. Economic burden of childhood autism spectrum disorders. Pediatrics. 2014;133(3):e520-9.
Levi, J., et al. F as in fat how obesity threatens America’s future : 2012. Washington, D.C.: Trust for America’s Health; 2012.
Li, Q., et al. Prevalence of Autism Spectrum Disorder Among Children and Adolescents in the United States From 2019 to 2020. JAMA Pediatr. 2022 Sep 1;176(9):943-945.
Manichanh, C., et al. The gut microbiota in IBD. Nat Rev Gastroenterol Hepatol. 2012;9(10):599-608.
Mattila, K., et al. Burden of illness and use of health care services before and after celiac disease diagnosis in children. J Pediatr Gastroenterol Nutr. 2013;57(1):53-6.
McCloud, E., et al. A medical nutrition therapy primer for childhood asthma: current and emerging perspectives. J Am Diet Assoc. 2011 Jul;111(7):1052–64.
Morimoto, Y., et al. Genetic Overlap Among Autism Spectrum Disorders and Other Neuropsychiatric Disorders. Autism Spectrum Disorders [Internet]. Brisbane (AU): Exon Publications; 2021 Aug 20. Chapter 6.
Most Recent Asthma Data. Centers for Disease Control and Prevention. Accessed 26 Mar 2026.
Organisation for Economic Co-operation and Development. Economic valuation of environmental health risks to children. Paris: Organisation for Economic Co-operation and Development; 2006. 310 p.p.
Perrin, J.M., et al. The increase of childhood chronic conditions in the United States. JAMA. 2007;297(24):2755-9.
Propp, P., et al. Prevention of asthma: where are we in the 21st century? Expert Rev Clin Immunol. 2013;9(12):1267-78.
Pulgaron, E.R. Childhood obesity: a review of increased risk for physical and psychological comorbidities. Clin Ther. 2013;35(1):A18-32.
Taylor-Black, S.A., et al. Prevalence of food allergy in New York City school children. Ann Allergy Asthma Immunol. 2014;112(6):554-6 e1.
Telford, C., et al. Estimating the costs of ongoing care for adolescents with attention-deficit hyperactivity disorder. Soc Psychiatry Psychiatr Epidemiol. 2013;48(2):337-44.
Trifonova, E.A., et al. Genetic and Pathogenic Overlaps Between Autism Spectrum Disorder and Alzheimer's Disease: Evolutionary Features and Opportunities for Drug Repurposing. Int J Mol Sci. 2025 Oct 16;26(20):10066.
Tuomi, T., et al. The many faces of diabetes: a disease with increasing heterogeneity. Lancet. 2014;383(9922):1084-94.
Van Meter, A.R., et al. What goes up must come down: the burden of bipolar depression in youth. J Affect Disord. 2013;150(3):1048-54.
Weiss, K.B., et al. Asthma’s impact on society: the social and economic burden. New York: M. Dekker; 2000. xv, 390 p.p.
Weiss, M.D., et al. Effectiveness outcomes in attention-deficit/hyperactivity disorder. J Clin Psychiatry. 2006;67 Suppl 8:38-45.
Zablotsky, B., et al. Estimated Prevalence of Children With Diagnosed Developmental Disabilities in the United States, 2014–2016. National Center for Health Statistics. NCHS Data Brief, No. 291, Nov 2017.
Resources
Books
Lambert, E., et al. A Compromised Generation: The Epidemic of Chronic Illness in America’s Children. Boulder, CO: Sentient Publications; 2010. xiv, 358 p.p.